

Image by Gerd Altmann from Pixabay
When and how can we safely reopen our economy?
This is the dilemma facing most governments around the World. Spatial data research is helping policymakers find some answers.
To this end, SafeGraph, a physical places data company, formed a COVID-19 Data Consortium. The Consortium is composed of over 3,000 researchers, non-profits, academic institutions, and government bodies who have free access to SafeGraph’s datasets.
Students at Stanford’s Future Bay Initiative are conducting research based on SafeGraph data to help the Bay Area develop a more accurate and informed approach to dealing with COVID-19. Derek Ouyang, a lecturer at Stanford University, mentors them.
Derek joined Daniel O’Donohue on the Mapscaping podcast for a conversation on the research.
Here’s an overview of what they discussed including:
- Components of the dataset
- Interesting insights from the research
- Challenges faced while working on the data
The dataset
SafeGraph’s data covers the whole U.S. However, Stanford’s research team reduces the data size to the areas of interest. These are; places within the 9 Counties in the Bay Area and the possible origins of visitors to these places.
SafeGraph’s dataset comprises:
Places data
Locations of where economic transactions happen in the U.S., e.g. retail establishments. It also includes building footprints and boundaries.
Patterns data
Monthly/ weekly data of the number of devices that have visited a specific location.
Visits data can be split into:
- Daily and hourly visit data
- Origin and destination of visitors
Safegraph also provides the device pool ratio because their data does not represent 100% of the population. In the U.S., the device pool ratio is 10:1. I.e. If there are 300 billion people in the U.S., then the monthly data that SafeGraph provides represents 30 million devices.
The ratio is used to extrapolate true visit counts from SafeGraph’s sample data.
Insights on the factors affecting disease spread
Having a reliably maintained and produced data set of places, and visit counts to and from those places are providing useful insights. Research with SafeGraph data is building confidence that there is a relationship between human movement, space, and disease spread.
Notwithstanding, SafeGraph’s visits (GIS) data doesn’t tell the whole story. It cannot capture all the factors that affect human wellbeing, human movement, public health, and disease spread. That said, spatial data is an effective communication tool to bring awareness to these other factors.
Below are some drivers of disease spread identified in the research.
Concentration and mixing
Apart from measuring the concentration of people in a certain time and space, SafeGraph data also allows measurements and observations regarding the degree of mixing between people from different locations.
For example, cramming 100 people in a specific space has a different disease spread outcome than having only 10 people in the same space observing social distancing. Likewise, 10 different Census Block Groups frequenting the same location versus only one Census Block Group frequenting the location is likely to reflect a degree of mixing that can also intensify disease spread.
In this way, SafeGraph data is used to trace movement back to specific Census Block Groups. Analysis of the patterns data shows the number of visits that a particular Census Block Group had to specific types of establishments in a week, and how long they were there.
Researchers then compare this data to the disease case growth for the particular Census Block Group some weeks in the future. The results are useful for the construction of movement and case growth indicators.
Access to open space
From an urban planning perspective, the access people have to backyard space for recreation is potentially a huge driver to how likely they are to go outside to parks or into the streets. People without access to open spaces are less likely to shelter-in-place leading to disease spread.
Consequently, there is a need for change in urban planning systems regarding public/ private access to open spaces.
Socio-economic demographics
Past census data about income, age distribution, race, people per household, and ethnicity, etc. in a Block Group has higher explanatory power on where disease case growth happens than SafeGraph visit data.
In the Bay Area, the variation in these socio-economic demographic factors has enabled researchers to explain over 75% of the variation in case growth in ZIP codes/Counties.
“… it appears to be the case that if you have higher income, however, that actually manifests, we are seeing that you have a greater ability to shelter in place and a greater ability to avoid the impact of COVID. Your age distribution in your Block Group, your language ability, in terms of communicating with health departments and government entities. These kinds of fixed community socio-economic demographic characteristics actually tell quite a bit of the story of what an inequitable distribution of impact looks like, not just in the Bay Area, but I am seeing through the Consortium, similar findings across the U.S.,…” (O’Donohue, 2020, 27:07)
Socio-economic demographic data is used to identify which potential community characteristics may lead to increased movement patterns, and thereafter to virus spread.
Systemic issues
The research is bringing systemic issues of inequality to the fore.
Today’s urban spatial arrangements are proof of this. Past spatial planning decisions affected the urban arrangements of housing, development, and transportation. These determined the geography of the places people live in. They work in the background, affecting their opportunities or livelihoods.
According to Derek, spatial data could be the magnifying glass we need for this history.
The research shows that there are higher disease cases and case growths in neighborhoods with predominantly people of color, people of low income, and people with pre-existing health conditions.
“So I would actually say that it’s not a sign of despair, that there are these systemic forces. I think that only doubles down my insistence that if we can put tools in the hands of students, policymakers, community activists to be able to tell the spatial stories here, then we can first just illuminate and make it very clear to everybody, just how inequality takes root in measured outcomes in our societies.” (O’Donohue, 2020, 31:46)
Challenges encountered
Even with good movement and case growth data, the researchers still face challenges when working on the datasets.
Data integration
In the Bay Area, Individual County health departments have dashboards that show daily cumulative cases by ZIP codes. In many other places in the U.S., the lowest case behavior and case growth data are at the County level.
On the other hand, SafeGraph’s places and patterns data are at the Census Block Group level.
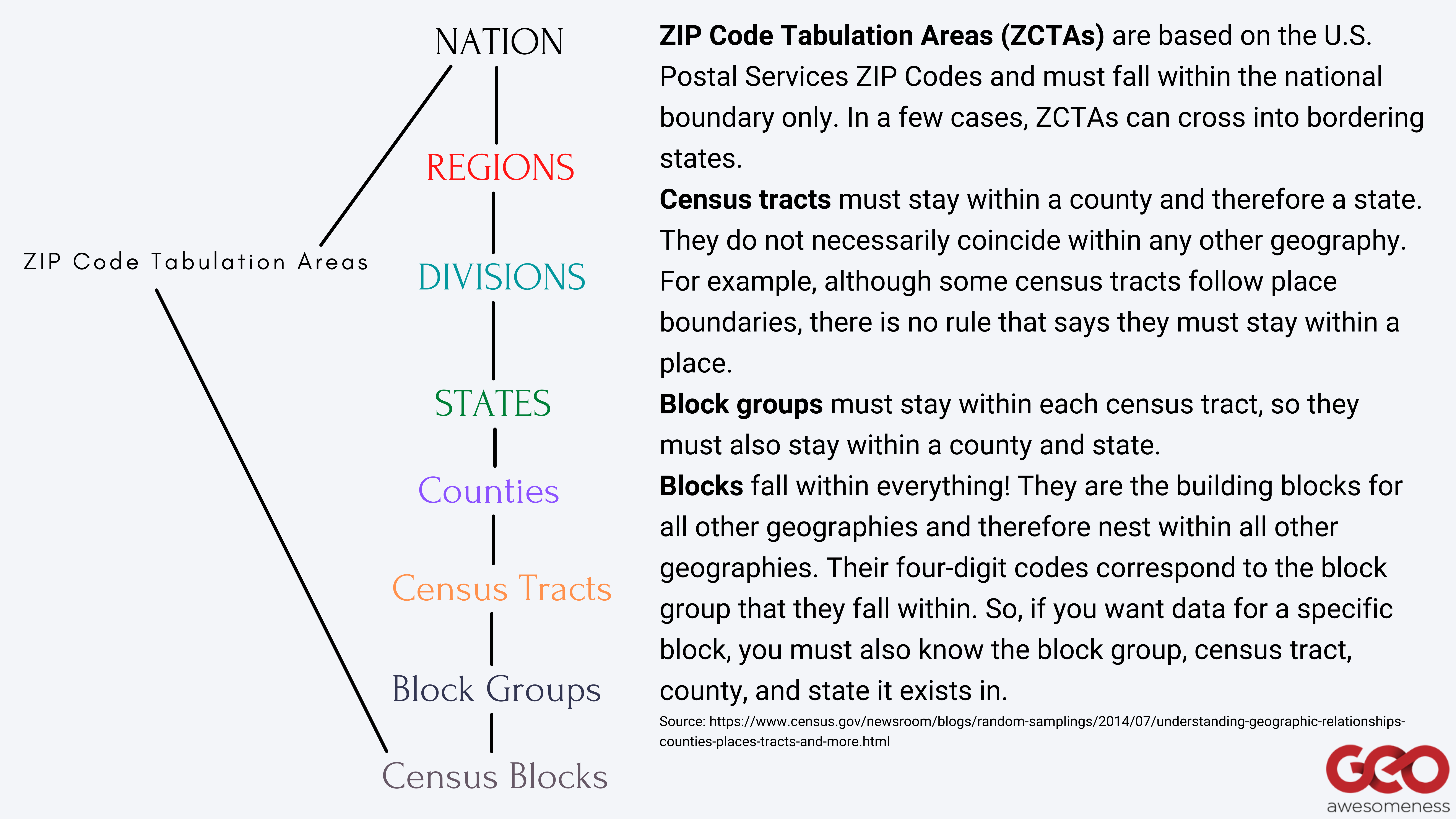
Hierarchy of census geographic entities in the U.S.
Ergo, there is a geospatial disconnect between case growth aggregations by ZIP code/ County, and the richer places and patterns data by Census Block Groups from SafeGraph. So, no matter how good SafeGraph data gets, if it cannot be linked back to the same granularity of case outcomes, there is an inability to refine certain questions.
For the Bay Area, the researchers scale up SafeGraph Census Block Group data to ZIP codes to enable comparison.
Lack of route tracking data
SafeGraph data is focused on indoor human movements. It doesn’t show the route people take from point A to point B. It just shows when and where they may have started from and when and where they end up.
According to Derek, there could be many important factors in the route.
For example, in places where public transit is common, buses and trains are important vehicles for disease spread. Unfortunately, this is invisible in SafeGraph data and would require incorporating insights by the collection of ridership data from a local transit agency or doing network analysis.
Nevertheless, because indoor transmission is likely greater than outdoor transmission, from a disease transmission perspective, indoor data is more important.
Aggregated data
SafeGraph provides movement behavior, aggregated up to the entire size of the business establishment or a Census Block Group. Therefore, you can only know averages or summaries for a large group of people. However, the disease works at the person-by-person level, making the dataset unuseful for individual contact tracing.
That said, the data is useful in showing the geospatial implications of where those interactions happened – whether they were in an indoor tight establishment or an outdoor park.
Next steps: Actionable intelligence
SafeGraph’s data and research is helping to create an objective record of the effects a specific activity or action has had on the disease spread. It is providing “actionable intelligence” — using data to identify the drivers we can change to arrive at the outcomes we want — around how governments can approach their COVID-19 response efforts.
The Consortium is improving the dataset, hence its explanatory power. With more refined insights, we can have more refined policy tools as well. A predictive tool with this kind of explanatory power is better than blindly making policy decisions about shutting off the entire economy or turning it all on at the same time.
Derek hopes that these predictive tools guide policymakers towards making more informed decisions.
Listen to the complete conversation on the Mapscaping Podcast.
You can find further details regarding the research on Stanford’s Future Bay Initiative COVID-19 Rapid Response Project page.
#Ideas


Next article


Remix cofounders
Seven years ago, Tiffany Chu met Dan Getelman, Sam Hashemi, and Danny Whalen while doing fellowships at Code for America – a nonprofit focused on empowering local governments. After months of slogging together on a grassroots hackathon project, they launched the beta version of a sketching tool that would allow transit planners to quickly design routes and share with the public.
In less than 24 hours, the prototype had gone viral and received media coverage from dozens of technology publications. And thus was born Remix, a platform to empower cities to plan the best possible transportation system.
Today, the California-based mapping platform is working with more than 350 local governments in 22 countries across five continents. It is being used to design hundreds of city transportation systems, impacting the lives of more than 240 million people worldwide.
And that impact is only going to increase because Remix has now been scooped up by Via, a leading software platform for public mobility that has more than 200 partners in 24 countries.
The $100 million cash and equity deal will see Remix and Via combining their strengths in planning and operations to collectively provide an end-to-end digital infrastructure for powering public mobility.

Chu, Remix CEO and Cofounder, says that joining forces with Via represents an incredible opportunity to tackle the biggest mobility challenges that cities must face in the decades to come. “Remix’s mission is to create more livable cities by expanding access within them. We are excited to join forces with Via, a company equally focused on increasing access by improving transportation options available to communities, and empowering cities with best-in-class technology for data-driven decision-making.”
Via, which started out as a ridesharing company in 2012 but has evolved to offer digital infrastructure for public mobility systems, hopes that the complementary capabilities of the two companies will help transportation planning, innovation, and operations teams respond to changing demands in real-time.
“We share a vision for working alongside our partners to create transit systems that are equitable, accessible, and efficient for riders and cities alike. Together, we have ambitious plans to invest in and expand the Remix product suite to offer enhanced capabilities for planning and bus scheduling and operations,” say Via Co-Founders Daniel Ramot and Oren Shoval.

